




Snoring is extremely common. In the 30-35 year old age group, 1 in 5 men and 1 in 20 women will snore. By 60 years of age, two-thirds of men will snore and almost half of all women!
Some people stop breathing for short durations (10 seconds or more) during their sleep. This is known as sleep apnea(OSA). This too is common and may affect a quarter of all men and a tenth of women between the ages of 30 and 60. Whilst sleep apnea on its own does not result in one 'dying in their sleep', it does raise the risk of high blood pressure, heart disease and diabetes.



Whilst many people snore, not everyone has sleep apnea. The following table lists some of the symptoms of sleep apnea. Ask your bed partner if you suffer from any of the night time symptoms
| Night time symptoms | Day time symptoms |
| Snoring, snorting, struggling to breathe, choking and breath-holding Thrashing in bed Frequent awakenings Frequently waking up to pass urine Palpitations | Feeling unrefreshed in the morning Excessive daytime sleepiness Forgetfulness and memory problems Difficult concentration Morning headaches Depression, irritability Impotence / sexual dysfunction |
In some patients, snoring is not associated with obstructive sleep apnea (OSA) but they suffer frequent arousals at night that disrupt the quality of their sleep. This is known as upper airways resistance syndrome (UARS). These patients are fortunate not to have obstructive sleep apnea but are described as "sleep snorers".
An assessment by an ENT surgeon is essential to assess the anatomy of your breathing passage from the nose to the windpipe. This involves nasal endoscopy where a slim flexible fibreoptic scope is passed through the nose into the upper airway. The surgeon will be able to assess if there is any obvious cause for airway obstruction, such as a long floppy soft palate, large tonsils or a large base of tongue.
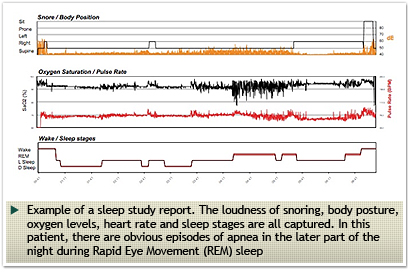
Most patients will then need an overnight sleep study. These studies may be conducted in the hospital or at home. During this study, your breathing pattern, snoring, oxygen levels in your blood, heart rate and brain waves are recorded for later interpretation. At The ENT Specialist, we have the facilities to perform WatchPat studies at home or a monitored sleep study within the hospital. The costs of these studies vary between $800 and $1800.
The treatment for snoring varies depending on whether there is co-existent sleep apnea (obstructive sleep apnea). The key to successfully treating snoring and sleep apnea is to establish the level of airway obstruction. The airway may be obstructed in the nose, at the level of the soft palate or lower down at the base of tongue.
| Airway Level | Cause of snoring | Treatment options |
Nose |
Enlarged nasal turbinates | Radiofrequency turbinate reduction (RFIT), Turbinoplasty |
| Deviated septum | Septoplasty, Septorhinoplasty | |
| Nasal polyps | Sinus surgery, polypectomy | |
| Enlarged adenoids | Adenoidectomy | |
Palate / Oropharynx |
Enlarged tonsils | Tonsillectomy, Tonsillotomy, Tonsil reduction |
| Long uvula | Uvulotomy | |
| Long, pendulous or bulky soft palate | UPPP), Coblator-assisted uvulopalatoplasty (CAUP), Cautery-assisted palatal stiffening operation (CAPSO) | |
Tongue base / Hypopharynx |
Large tongue | Radiofrequency tongue reduction, Transoral Robotic Surgery (TORS), Genioglossus advancement, Median glossectomy |
| Recessed jaw (Retrognathia) | Maxillo-mandibular advancement | |
| Floppy, weak or retroverted epiglottis | Epiglottidectomy, epiglottopexy, epiglottoplasty |
In patients with severe sleep apnea, continuous positive airway pressure (CPAP) may the only treatment that is effective. To improve compliance with CPAP, nasal surgery such as septoplasty or turbinoplasty may be undertaken to improve nasal patency.
